Effectiveness of 222nm Far UVC Light on Disinfecting SARS-CoV-2
Background
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19), has emerged as a serious threat to human health worldwide. Efficient disinfection of surfaces contaminated with SARS-CoV-2 may help prevent its spread. This study aimed to investigate the in vitro efficacy of 222-nm far-ultraviolet light (UVC) on the disinfection of SARS-CoV-2 surface contamination.
Methods
We investigated the titer of SARS-CoV-2 after UV irradiation (0.1 mW/cm2) at 222 nm for 10-300 seconds using the 50% tissue culture infectious dose (TCID50). In addition, we used quantitative reverse transcription polymerase chain reaction to quantify SARS-CoV-2 RNA under the same conditions.
Results
One and 3 mJ/cm2 of 222-nm UVC irradiation (0.1 mW/cm2 for 10 and 30 seconds) resulted in 88.5 and 99.7% reduction of viable SARS-CoV-2 based on the TCID50 assay, respectively. In contrast, the copy number of SARS-CoV-2 RNA did not change after UVC irradiation even after a 5-minute irradiation.
Conclusions
This study shows the efficacy of 222-nm UVC irradiation against SARS-CoV-2 contamination in an in vitro experiment. Further evaluation of the safety and efficacy of 222-nm UVC irradiation in reducing the contamination of real-world surfaces and the potential transmission of SARS-CoV-2 is needed.
Severe acute respiratory syndrome coronavirus (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19), has emerged as a serious threat to human health worldwide.SARS-CoV-2 is mainly transmitted through infected respiratory droplets and close contact with infected people. Recent studies showed that SARS-CoV-2 can remain viable for days on surfaces under controlled experimental conditions.Furthermore, surfaces in hospitals treating patients with COVID-19 were found to be contaminated by SARS-CoV-2, suggesting that the hospital environment could be a potential medium of transmission. Therefore, if environmental disinfection is not effective, SARS-CoV-2 may spread widely and cause nosocomial infections.
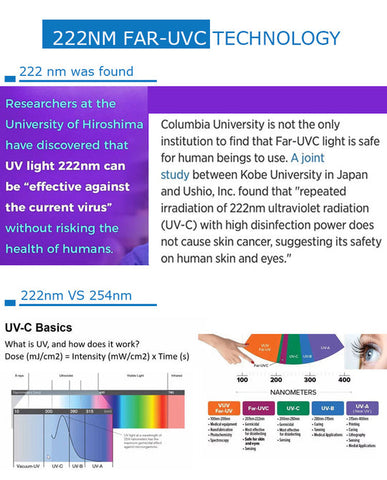
Recently, ultraviolet (UV) light disinfection systems have been increasingly used in health care settings in an attempt to decrease the transmission of nosocomial pathogens and prevent health care-associated infections.Most UV disinfection systems use germicidal lamps emitting UV radiation C (UVC) around 254 nm. However, it is well known that 254-nm UVC is harmful to the skin and eyes. Previous reports demonstrated that 222-nm UVC light, belonging to far-UVC (207-222 nm), has the same highly effective germicidal properties as 254-nm UVC; however, it is less harmful to the skin and eyes than 254-nm UVC because far-UVC light has a very limited penetration depth in the skin or eye. In addition, previous studies have reported that low dose of 222-nm UVC inactivated aerosolized H1N1 influenza virus and human coronaviruses alpha HCoV-229E and beta HCoV-OC43. Although there are a few reports about the effectiveness of UV disinfection on SARS-CoV-2,the effect of 222-nm UVC on SARS-CoV-2 is poorly understood. The aim of this study was to investigate the in vitro efficacy of 222-nm UV disinfection of SARS-CoV-2 contamination.
METHODS
Cells and virus
VeroE6/TMPRSS2 cells (African green monkey kidney-derived cells expressing human TMPRSS2, purchased from Japanese Collection of Research Bioresources (JCRB) Cell Bank, JCRB1819)were propagated in Dulbecco's modified Eagle's minimum essential medium (DMEM, Invitrogen) supplemented with 10% fetal calf serum (FCS; Biosera, Kansas City, MO), penicillin G (100 units/mL, Meiji Seika Pharma, Tokyo, Japan), and streptomycin (100 µg/mL, Meiji Seika Pharma). The cells were cultured at 37°C in 5% CO2. SARS-CoV-2 2019-nCoV/Japan/AI/I-004/2020 strain was provided by the National Institute of Infectious Diseases, Japan. To prepare virus suspensions, VeroE6/TMPRSS2 cells were infected with the virus and incubated in DMEM. When cytopathic effects were fully developed, the culture supernatant was harvested and filtered through a 0.45-µm filter. The virus titer was determined by the standard 50% tissue culture infectious dose (TCID50) method and expressed as TCID50/mL, as described previously.
Viral suspensions (100 µL) containing ca. 5 × 106 TCID50/mL were loaded onto a sterile polystyrene plate (9-cm diameter) and spread into a circle with a diameter of approximately 7 cm. The inoculum was allowed to dry under sterile laminar flow in a biosafety cabinet at room temperature. A total of 5 plates were prepared in triplicate for a nonirradiated control and for 222-nm UV disinfection for 10, 30, 60, and 300 seconds. All experiments with SARS-CoV-2 virus were performed in a biosafety level 3 (BSL3) containment facility at Hiroshima University. All experimental results are reported as means across 3 replicates.
222-nm UVC disinfection
The Care222 (Ushio Inc., Tokyo, Japan) UVC emitting device used in this study was a 222-nm krypton-chloride (Kr-Cl) excimer lamp module. The lamp contains an optical filter that removes essentially all but the dominant 222-nm emission wavelength.For 222-nm UVC irradiation, the Care222 was placed 24 cm above the surface of the plates, and the radiation intensity at the surface of the plates was 0.1 mW/cm2, as measured with a recently calibrated Unimeter SNK005 meter (Ushio Inc., Tokyo, Japan). After irradiation for each treatment time, the control and treated plates were washed with 1 mL of phosphate-buffered saline for 1 minute and the virus-containing phosphate-buffered saline was collected in a test tube for analysis.
TCID50
We used the standard TCID50 method to determine virus titer for the collected viral samples from each plate as previously described.Log10 TCID50/mL reductions were calculated by comparing the log10 TCID50/mL values recovered from plates after 222-nm UVC irradiation with those from control (nonirradiated) plates.
Quantitative reverse transcription PCR (RT-qPCR)
SARS-CoV-2 RNA was extracted from the collected viral samples from each plate using a NucleoSpin RNA Virus kit (MACHEREY-NAGEL GmbH & Co. KG., Düren, Germany) following the manufacturer's protocol. Conventional RT-qPCR for the specific amplification of the nucleocapsid (N) gene of SARS-CoV-2 was performed using the One Step PrimeScript III RT-qPCR mix (Takara Bio Inc., Kusatsu, Japan) according to the manufacturer's protocol. The following sets of primers and probe were used: forward primer (2.4 μM), 5′-AAA TTT TGG GGA CCA GGA AC-3′; reverse primer (3.2 μM), 5′-TGG CAG CTG TGT AGG TCA AC-3′; and 0.4 μM probe, 5′-FAM-ATG TCG CGC ATT GGC ATG GA-BHQ-3′. Thermal cycling was carried out as follows: reverse transcription at 52 °C for 5 minutes, initial denaturation at 95 °C for 10 seconds, 45 cycles of denaturation at 95 °C for 5 seconds, and a final annealing/extension at 60 °C for 30 seconds.
RESULTS
The results of the TCID50 assay and RT-qPCR are shown in Table 1. Three mJ/cm2 of 222 nm UVC light (0.1 mW/cm2 for 30 seconds) reduced viable SARS-CoV-2 (99.7% reduction) to undetectable levels based on the TCID50 assay. In contrast, the copy number of SARS-CoV-2 RNA did not change after UV irradiation compared to that of the nonirradiation control, even after the maximum 300 s exposure (cycle quantification (Cq), 17.02-18.32).
Table 1. Efficacy of 222-nm UVC light (0.1 mW/cm2) on reducing viable SARS-CoV-2
|
|
UVC irradiation time |
||||
|
|
Control |
10 seconds |
30 seconds |
60 seconds |
300 seconds |
|
Mean viable SARS-CoV-2 (TICD50/mL) (SD) |
2.05 ± 1.21 × 104 |
2.34 ± 0.86 × 103 |
6.32 ± 0.0 × 101 |
6.32 ± 0.0 × 101 |
6.32 ± 0.0 × 101 |
|
Log reduction |
|
0.94 |
2.51 |
2.51 |
2.51 |
|
Mean SARS-CoV-2 RNA href="#tb1fn1" * (copies/test) (SD) |
2.12 ± 0.27 × 107 |
5.75 ± 0.82 × 107 |
3.41 ± 1.08 × 107 |
2.95 ± 0.41 × 107 |
3.03 ± 1.73 × 107 |
SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TCID50, 50% tissue culture infectious dose; SD, standard deviation.
⁎
SARS-CoV-2 RNA was measured by quantitative reverse transcription PCR.
DISCUSSION
The results of this study demonstrated that 222-nm UVC irradiation at 3 mJ/cm2 (0.1 mW/cm2 for 30 seconds) resulted in a 99.7% reduction of viable SARS-CoV-2 based on the TCID50 assay. Previous reports showed that a low dose of 222-nm UV inactivated several viruses, although the treated viruses were aerosolized; 2 mJ/cm2 of 222-nm UV inactivated >95% of H1N1 aerosolized influenza virus.14 In addition, 1.7 and 1.2 mJ/cm2 of 222-nm UV inactivated 99.9% of aerosolized human coronaviruses alpha HCoV-229E and beta HCoV-OC43, respectively.Previous report showed that the viral titer of SARS-CoV-2 was reduced on a plastic plate over time.3 The decrease of the viral titer of the control plate by dry conditions may have resulted in the plateau of the virus killing at a very low UV dose of 3 mJ/cm2. A few previous reports showed the effectiveness of UV disinfection on SARS-CoV-2; however, it is difficult to compare the result of this study to that of previous studies because the wavelength of UV or the experimental conditions are different. In contrast to the viable SARS-CoV-2, the copy number of SARS-CoV-2 RNA determined by RT-qPCR was not reduced even after 30 mJ/cm2 (0.1 mW/cm2 for 300 seconds) of 222-nm UVC irradiation. Because our results of RT-qPCR showed that the almost same number of RNA copies with a range of Cq values from 17.02 to 18.32, we believe that our RT-qPCR assay worked well. Recent studies have reported on SARS-CoV-2 contamination in hospital environments as determined by RT-qPCR.However, our study suggests that this technique does not accurately reflect viable SARS-CoV-2 contamination. Rather, the TCID50 assay should be used to detect viable SARS-CoV-2 contamination after UV disinfection.
To protect health care workers and to help stop the spread of SARS-CoV-2, more thorough prevention and control practices are needed. Since COVID-19 has become a pandemic and there are asymptomatic patients,attention is being focused on environmental disinfection in public spaces beyond health care settings in which many people come into contact with various surfaces. Although the most common UV disinfection system in use is a germicidal lamp emitting around 254-nm UVC,it is well known that this wavelength is harmful to the skin and eyes. Thus, the germicidal lamp UV disinfection systems can mainly only be used in unoccupied spaces. In contrast, recent studies have shown that 222-nm UVC is less harmful than 254-nm UVC because far-UVC light has a very limited penetration depth in the skin or eyes and it is also an efficient anti-microbial technology.Therefore, a 222-nm UVC disinfection system could be used in occupied public spaces including a hospital room, which is occupied by patients and frequented by health care workers and possibly, visitors. However, further study about the safety and efficacy of 222-nm UVC irradiation in occupied space is needed.
One limitation of our study is that we only investigated the in vitro efficacy of 222-nm UV irradiation on SARS-CoV-2 contamination. We did not evaluate this technology in a real-world setting, such as a surface counter-top.
CONCLUSIONS
In conclusion, our study demonstrated the effectiveness of 222-nm UVC irradiation on viable SARS-CoV-2. Our results suggest that this technology could be used for infection prevention and control against COVID-19, not only in unoccupied spaces but also occupied spaces. Further evaluation of the safety and efficacy of 222-nm UVC irradiation in reducing the contamination of real-world surfaces and the transmission of SARS-CoV-2 is needed.